 +91 8248827895 |
+91 8248827895 |  absolutevitalhealth@gmail.com
absolutevitalhealth@gmail.com
Sciatica Pain
A lumbosacral radicular syndrome (LSR) is characterized by a radiating pain in one or more regions in the lower body;
It may or may not be accompanied by other nerve irritation symptoms and/or symptoms of decreased sensation or muscle power. It is caused by nerve root irritation/inflammation and/or compression.
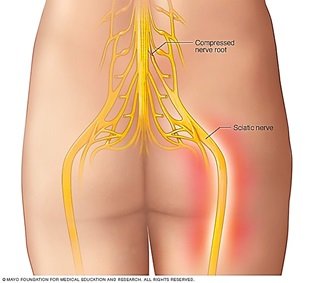
The lumbosacral radicular pain is presumably the most commonly occurring form of neuropathic pain which is also referred to as sciatica, or nerve root pain.
The terms radicular pain and radiculopathy are also sometimes used interchangeably, although they certainly are not synonyms.
In the case of radicular pain, only radiating pain is present, while in the case of radiculopathy, sensation loss and/or reduction in muscle power can be observed.
The most important risk factors are: being male, obesity, smoking, history of low back pain, anxiety and depression, work which requires lengthy periods of standing and bending forward, heavy manual labour, lifting heavy objects, and being exposed to vibration.
Pain completely or partially resolves in 60% of the patients within 12 weeks of onset. However, about 30% of the patients still have pain after 3 months to 1 year, which affects the quality of life. Apparently, the female population with Sciatica (LRS) has a considerably worse outcome compared with the male population.
What is the most common reason for Sciatica?
In patients under 50 years of age, a herniated disc is the most frequent cause of Sciatica. After the age of 50, radicular pain is often caused by age related degenerative changes in the spine.
How does the Sciatica pain feel and what aggravates/relieves the pain?
The patient may experience the radiating pain as sharp, dull, piercing, throbbing, or burning. Pain caused by a herniated disc classically increases by bending forward, sitting, coughing, or (excessive) stress on the lumbar discs and can be avoided by lying down or sometimes by walking.
Where pain is from a lumbar spinal canal stenosis, it can typically increase when walking and improve immediately upon bending forward.

How is the Sciatica pain clinically diagnosed?
Straight leg raising test is used to diagnose LSR. If radicular pain can be elicited under 60°, there is a large chance that a lumbar herniated disc is present. When L4 nerve root is involved knee reflex is diminished, foot inversion is weak. When L5 is involved, there is decreased ankle dorsiflexion, and weak toe extension, when S1 involvement is present then plantar flexion is decreased.
What are the other causes of Sciatica?
The most common causes are slipped disc and spinal canal stenosis. Other causes include
- Entrapment of the sciatic nerve under a tightened muscle such as Piriformis causing a syndrome called piriformis syndrome. When this tightened muscle gets relaxed the Sciatica gets relieved.
- Spondylolisthesis is a condition that occurs when one vertebral body slips with respect to the adjacent vertebral body causing radicular or mechanical symptoms or pain. It is graded based on the degree of slippage of one vertebral body on the adjacent vertebral body
- Pelvis injury or bone fracture


What imaging is required to diagnose Sciatica?
Medical imaging, primarily magnetic resonance imaging (MRI), can confirm the presence of a herniated disc; this technique is preferred because of the better visualization of soft tissues and the lower radiation dose.
In the event of an unclear clinical picture or in the absence of radiological evidence for radicular complaints, electromyography (EMG)/nerve conduction studies (NCS) can be performed to differentiate lumbar radicular syndrome from peripheral neuropathy.
How is Sciatica treated?
Medically treated with Non steroidal Anti inflammatory Drugs/Nerve Strengthening medications followed by exercise therapy.

What is the need for Epidural Steroid?
If the pain doesn’t get relieved in 4-6weeks time or if the pain is severe affecting the patients’ quality of life, then Epidural Steroid would be effective in most of these patients.
The logic of epidural corticosteroid administration rests on the anti-inflammatory effect of the corticosteroids, which are administered directly onto the inflamed nerve root. There are three approaches: interlaminar, transforaminal, and caudal.
Transforaminal steroid injection is delivering the steroid to the epidural space nearer to the nerve roots and hence more effective than interlaminar.

When is Caudal Epidural Steroid indicated?
Caudal epidural steroid is indicated when the lower lumbar and/or sacral nerve are affected or when there is spinal canal stenois. Here the steroid in injected in the lower spinal canal which provide effective relief from LSR.
What is selective lumbar nerve root injection?
When disc prolapse compresses a specific nerve root, the steroid can be deposited near that particular nerve root alone under fluoroscopic image guidance.
Does the pain come back after steroid injection?
All steroid injections are followed by a short period of rest and then they should start doing spinal exercises, to strengthen the core muscles, which will help in preventing the pain from coming back.

Frequently Asked Questions
Sciatica can be due to various reasons ranging from a severe disc prolapse to a simple muscle strain. So depending upon the cause, the treatment varies from transforaminal epidural steroid to simple outpatient prolotherapy. So to know which treatment is best for your sciatica, kindly contact Absolute Vital Health at Aikiya Healthcare.
Dr.Ayshvarya Ramalingam has years of experience in treating patients with sciatica, from severe disc prolapse causing radiculopathy, helping them walk back home without surgery. She has identified patients who can be treated with simple medications instead of procedures. Many patients with sciatica have benefitted with right medical treatment.
Pain on one side of the buttock can be due to muscle strain, sacroiliac joint pathology, facet joint pain or nerve pain. The treatment varies depending upon the cause of the pain. If you are suffering from one sided buttock pain, kindly visit Absolute Vital Health at Aikiya Healthcare to find out the cause of pain and relevant treatment options.
Sitting for long hours can itself cause tension in the muscles such as hamstrings and calf muscles. The nerve that passes through these tensed and contracted muscles can get compressed mimicking sciatica. Sitting for long hours can increase disc pressure resulting in a prolapse which may compress a nerve at its root level causing sciatica. If you want to get evaluated for your low back pain, kindly book an appointment with Dr.Ayshvarya Ramalingam and get yourself treated.
Sciatica can be prevented by lifestyle changes which support a healthy spine and muscle health. Regular yoga stretches are good nutrition for the spine. Lifestyle changes such as avoiding sitting for long hours, moving from your couch every 30 mins, proper hydration, regular walking and stretching of muscles. All these can prevent you from getting sciatica in future. If you are already suffering from sciatica, book an appointment with Dr.Ayshvarya Ramalingam, and get the best sciatica treatment.